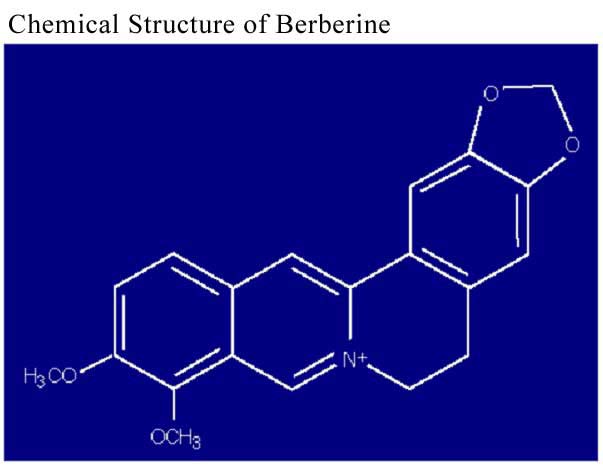
Berberine
is a plant alkaloid with a long history of medicinal use in boty Ayurvedic and
Chinese medicine. It is present in Hydrastis Canadensis(Goldenseal), Coptis chinensis
(Coptis or goldenthread), Berberis aquifolium (Oregon grape), Berberis Vulgaris
(Barberry), and Berberis aristata (tree turmeric). The berberine alkaloid can
be found in the roots, rhizomes, and stem bark of the plants. Berberine extracts
and decoctions have demonstrated significant antimicrobial activity against a
variety of organisms including bacteria, viruses, gungi, protozoans, helminthes,
and Chlamydia. Currently, the predominant clinical uses of berberine include bacterial
diarrhoea, intestinal parasite infections, and ocular trachoma infections.
The
pharmacologic actions of berberine include metabolic inhibition of certain organisms,
inhibition of bacterial enter toxin formation, inhibition of intestinal fluid
accumulation and ion secretion, inhibition of smooth muscle contraction, reduction
of inflammation, platelet aggregation inhibition, platelet count elevation in
certain type of thrombocytopenia, stimulation of bile and bilirubin secretion,
and inhibition of ventricular tachyarrhythmias.
Much
of the research on berberine has focused on its use in cases of diarrhoea, including
that caused by Vibrio cholerae1-4 and Escherichia coli.2,3,5,6 Studies have demonstrated
a direct antibacterial effect of berberine against V. cholerae,1 and berberine
has been shown to inhibit the intestinal secretory response caused by E. coli
heat-stable enterotoxin (ST)22 and V. cholerae enterotoxins.2-4 In addition to
its direct antimicrobial action, berberine has also been shown to block the adherence
of Strep. pyogenes6 and E. coli7 to erythrocytes and epithelial cells. Thus, it
is possible berberine exerts an antibiotic effect, even against organisms that
do not exhibit in vitro sensitivity to the alkaloid.
A
series of 63 adult males with enterotoxigenic E. coli (ETEC) diarrhoea of similar
clinical characteristics were serially assigned to either an experimental group
or a control group by use of a random number table. Thirty-three people were given
a single dose of 400 mg berberine sulfate (BS) orally. The control group received
no treatment. Both groups received IV rehydration therapy, and were observed for
a period of 24 hours. During the total observation period, the experimental group
had a 48% reduction in mean stool volumes compared with the controls (p<0.05).
Also, when compared with the control group, significantly more of those receiving
BS stopped having liquid diarrheal stools during the observation period (42% vs.
20%, p<0.05).2
Berberine
has been shown to inhibit the intestinal secretory response due to cholera toxins.
Using a ligated rabbit intestinal loop model, Sack and Froehlich were able to
demonstrate a significant suppression of the intestinal secretory response following
exposure to V. cholerae crude enterotoxin. This effect was similar whether the
berberine was administered immediately prior to the cholera toxin, or as long
as four hours after exposure (p<0.02), and did not require direct mucosal contact
to be effective. In discussing their results, the authors note, "...it is
also of clinical importance that berberine has not been reported to have significant
side effects at the doses used clinically in humans (5 to 10 mg/kg per day orally)..."3
In patients
with cholera, analysis by factorial design equations revealed a reduction in diarrheal
stools by one liter and a reduction in cyclic adenosine monophosphate concentrations
in stools by 77% in the groups given berberine. In other studies of diarrhoea
due to Vibrio cholerae and ETEC, berberine (200 mg) reduced stool volumes 30-50%
in diarrhoeal patients without significant side effects. Berberine's effectiveness
in reducing water and electrolyte secretions induced by ST and cholera toxin appear
to be enhanced in a dose-dependent manner.
While
the precise mechanism of action of berberine remains to be elucidated, in addition
to the direct bacteriocidal action, several other mechanisms may account for its
ability to inhibit infectious diarrhoea. Metabolic inhibition of certain organisms,
inhibition of the formation of toxins, direct antagonism of the toxins, inhibition
of intestinal ion secretion, and inhibition of smooth muscle contraction may all
play a role in this plant extract's antidiarrhoeal activity.
The antidiarrheal
properties of berberine may be mediated, at least in part, by its ability to delay
small intestinal transit time. Berberine has been shown to block muscarinic receptors
and to exhibit a noncompetitive inhibition of the contractile response induced
by acetylcholine, thus acting to inhibit spontaneous peristalsis in the intestine.
In animal studies, the transit of the small intestine was significantly delayed
at 15 and 100 minutes after the highest doses of BS. In humans, 1.2 grams of berberine
significantly delayed small intestine transit time after an oral dose.
Berberine
sulfate has been shown to possess growth inhibitory activity against Giardia lamblia,
Trichomonas vaginalis, and Entamoeba histolytica in axenic culture. It was observed
that the crude extract was more effective than the salt. The greater inhibitory
activity of the crude extract may be due to the cumulative contributions of berberine
along with other alkaloids and pharmacologically active constituents.
Subbaiah
and Amin reported that BS was effective against the protozoan Entamoeba histolytica
in a study that evaluated both in vitro and in vivo outcomes. In vitro testing
indicated berberine "...is amebicidal at a concentration of 0.5-1.0 mg/ml,
and that it acts rapidly." After addition of berberine, morphological changes
could be observed in the trophozoites, including encystation, degeneration, and
lysis. Preliminary results also indicated berberine may be cysticidal as well.
Golden hamsters
were given either 3 or 5 mg/kg body weight of BS orally three times at 4-hour
intervals. The initial dose was given prior to intrahepatic infection with E.
histolytica, the second at the time of infection, and the third 4 hours later.
At 5 mg/kg, 100% of the animals showed normal livers upon necropsy four days later
with no trophozoites found, while at 3 mg/kg, 33% showed small hepatic abscesses.
In the control group, 75% of the animals demonstrated liver abscesses with trophozoites.
Similar results were found in rats infected with E. histolytica via the intestinal
tract, where the control group developed intestinal amebiasis while the berberine
group did not.
Giardia
lamblia, another common protozoan infecting humans, has also been found to be
sensitive to berberine. Nearly 20 years ago, Choudhry et al reported on 40 children
(ages 1-10 years) infected with Giardia, who received either B-vitamin syrup (which
they termed "a placebo"), berberine (5 mg/kg/day) or metronidazole (10
mg/kg/day). The substances were administered in three divided doses for 6 days.
Following the placebo, 15% of the subjects became symptom-free and 25% demonstrated
no Giardia in the stool. After taking berberine, 48% became asymptomatic and 68%
were Giardia-free upon stool analysis. All of those receiving metronidazole showed
no Giardia remaining, but only 33% of them had resolution of symptoms.
In another
study, a total of 137 children (ages 5 months to 14 yr, mean age 5 yr) with documented
giardiasis were given either 5 mg/kg/day or 10 mg/kg/day of berberine in divided
doses, for a period of either 5 or 10 days. They were then compared with 242 subjects
placed on conventional therapy, including 88 who received metronidazole (20 mg/kg/day
for 5-7 days). Ninety percent of those receiving berberine (10 mg/kg/day for 10
days) had negative stool specimens after 10 days, and 83% remained negative one
month later, which compared favourably with those treated with metronidazole (95%
and 90%, respectively). The author concludes by citing berberine's "...convenience
of administration and freedom from unpleasant side effects."
In visceral leishmaniasis, berberine has also shown significant effectiveness.
One percent BS inoculated intralesionally on four occasions at weekly intervals
was found to be highly effective against cutaneous leishmaniasis in domestic dogs.
Berberine was evaluated in golden hamsters infected with L. donovani amastigotes
in two separate trials. In the 8-day model, berberine was administered intraperitoneally
at 50 and 100 mg/kg/day for 4 days beginning on the third day following infection,
and compared with infected controls. On necropsy, the liver parasite burden was
determined: the 50 and 100 mg/kg/day berberine groups showed 0.86 +/- 0.09 and
0.65 +/-0.10 cells x 108 respectively, compared with infected
controls which showed 1.67 +/- 0.63 cells x 108 (p<0.05).
In
an extended 60-day model, uninfected hamsters, infected controls, and infected
animals treated with berberine were observed. The experimental group was administered
berberine intraperitoneally (50 mg/kg/day) for 5 days, beginning 1 month after
infection. After a five-day interval the berberine course was repeated. Upon evaluation,
the berberine group was found to have a reduction in both liver and spleen parasite
burden of 90% compared to infected controls (p<0.001). In addition, leukocyte
counts were normalized: normal hamsters = 9343 +/- 1627; infected controls = 2862
+/- 534; berberine group = 7112 +/- 13.7 cells/mm3 (p<0.001).
"In vivo, berberine was found to be as effective as pentamidine and had the
advantage of being better tolerated."
Aqueous
solutions of berberine have also been employed in cases of ocular infections,
especially those resulting from Chlamydia trachomatis. Fifty-one people attending
an out-patient eye clinic having stage I or stage II trachoma lesions were recruited
into the study. Subjects were divided into three groups: Group I received 0.2%
berberine chloride eye drops, 2 drops per eye 3 times daily for 3 weeks; Group
II received eye drops containing 0.2% berberine chloride plus 20% sulfacetamide
according to the same schedule; Group III received eye drops containing only 20%
sulfacetamide.
After
3 weeks, subjects in Group III had a slightly better clinical improvement as judged
by conjunctival congestion, number of follicles and papillary reaction. The conjunctival
scrapings of all subjects in Group III still tested positive for C. trachomatis,
and these subjects were likely to have a relapse of symptoms. Subjects in Groups
I and II showed a significant improvement in symptoms compared to their initial
examination, and following the experimental period had only very mild symptoms
remaining. All subjects in Groups I and II had conjunctival scrapings which were
negative for C. trachomatis. Those in Groups I and II had no incidence of relapse
up to one year later.
To
further determine if these anti-trachoma effects were related to direct anti-chlamydial
properties of berberine or to host-mediated factors, a series of in vitro and
in vivo experiments were carried out using chick embryos. Three different C. trachomatis
isolates were incubated in vitro with 0.2% berberine chloride prior to inoculation
into chick embryos. A different set of embryos was initially infected with the
C. trachomatis isolates, and then subsequently given 3 doses of 0.2% berberine
chloride. The in vitro incubation of C. trachomatis with berberine had no effect
in reducing the lesion scores or mortality of the organism, whereas administration
of the berberine to infected
The
clinical serological response to topical treatment of trachoma with berberine
was studied in 32 microbiologically confirmed cases. Efficacy of berberine 0.2%
when compared to sulfacetamide 20% was found to be superior in both the clinical
course of trachoma and in achieving a fall in serum antibody titers against Chlamydia
trachomatis.
Experimental
results in animals and clinical trials in humans suggest intravenous berberine
may be effective in preventing the onset of reentrant ventricular tachyarrhythmias
and sudden coronary death after myocardial ischemic damage.
In vitro, berberine
increases, in a concentration-dependent manner, the action potential duration
in canine Purkinje and ventricular muscle fibers without effecting other parameters
of the action potential. The authors suggest, "...berberine exerts Class
III antiarrhythmic and proarrhythmic actions in cardiac muscle of the dog in vitro."
In 18 dogs
with ischemic left ventricular failure, berberine was able to improve impaired
left ventricular function by its positive inotropic effect and mild systemic vasodilation.Berberine
increased coronary artery flow of anesthetized open-chest canines and isolated
guinea pig hearts. Rabbits were protected by berberine from ischemic ECG changes
caused by posterior pituitary hormones. Spasm of isolated swine coronary arterial
rings was prevented and treated effectively by berberine.
In humans, 12
patients with refractory congestive heart failure were studied before and during
berberine intravenous infusion at rates of 0.02 and 0.2 mg/kg per min for 30 minutes.
The lower infusion dose produced no significant circulatory changes, apart from
a reduction in heart rate (14%). The 0.2 mg/kg per min dose elicited several significant
changes. A 48% decrease in systemic and a 41% decrease in pulmonary vascular resistance,
along with a 28% decrease in right atrium and 32% decrease in left ventricular
end-diastolic pressures were observed. Measurable increases in cardiac index (45%),
stroke index (45%), and left ventricular ejection fraction (56%) were found. Also
noted were increases in hemodynamic and echocardiographic indices of left ventricular
performance and a decrease in arteriovenous oxygen uptake (28%) with no changes
in total body oxygen uptake, arterial oxygen tension, or hemoglobin dissociation
properties.
The
effects of berberine on 100 individuals with ventricular tachyarrhythmias observed
with 24 to 48 hour ambulatory monitoring has also been reported. The results indicate
62% of patients had 50% or greater, and 38% of patients had 90% or greater suppression
of ventricular premature contractions (VPC). No severe side effects were observed;
however, mild gastro-enterologic symptoms were reported by some patients.
Several mechanisms
have been proposed to explain the observed effects of berberine. Zhou observed
berberine works as a Ca2+ channel agonist, while Hua and Wang suggest the antiarrhythmic
action of berberine might be due to its potassium channel blocking effects. Experiments
on the rat fundus indicate berberine inhibits the entry of extracellular calcium
into the cell. Evidence also suggests berberine, by reducing tyrosine hydroxylase
activity, has an inhibitory effect on catecholamine biosynthesis.
Among
berberine's multiple pharmacological actions is anti-inflammatory activity. In
vitro, a consistent and progressive inhibitory influence of berberine with increasing
concentrations was identified with all mitogens and was most pronounced with pokeweed
mitogen. Berberine (20 mg/kg/d) inhibited platelet aggregation and platelet adhesion
induced by ADP, arachidonic acid, and collagen in rats. The same dose of berberine
also inhibited thrombus formation.
Berberine
may inhibit the release of arachidonic acid from cell membrane phospholipids and
exerts an effect on arachidonic acid metabolites. Berberine dose-dependently inhibits
collagen-, ADP-, and arachidonic acid (AA)-induced thromboxane A2 release from
platelets. Berberine given intravenously lowers rabbit plasma level of PGI2.49
While an extract of the bark from Berberis aquifolium has been shown to inhibit
5-lipoxygenase with an IC50 value of 50 microM, berberine has not been shown to
exert a significant inhibitory effect.
In
experimental animals, berberine has been shown to reduce the purging effects of
castor oil or Cassia angustifolia leaf, significantly inhibit drug-induced vascular
permeability, and inhibit
drug-induced
swelling in a dose-dependent manner. Berberine has shown an inhibitory effect
against induced ear edema in experimental animals.
There
has been increased interest in lowering blood cholesterol, and especially LDL-cholesterol,
as a means of curtailing the high rates of heart attack and stroke. In addition
to recommended dietary changes, many people are prescribed statin drugs for this
goal. The statin drugs are powerful, frequently effective, and may have other
benefits, though they also pose certain risks. During the 1990s, the Chinese herb
material "red rice yeast" (Monascus purpureus) was sold in the U.S.
as a natural supplement that contains, as one of its active ingredients, small
amounts of lovastatin, one of the widely used statin drugs (it also contains several
related compounds that contributed to the cholesterol lowering action). After
prolonged legal disputes between the supplement providers, the drug companies,
and the FDA about its content of the drug substance, the sale of red rice yeast
and its extracts as natural cholesterol lowering agents was banned.
It was reported
recently that berberine lowers cholesterol through a mechanism different than
that of the statin drugs, suggesting potential use both as an alternative to the
statins and as a complementary therapy that might be used with statins in an attempt
to gain better control over cholesterol. In a controlled Chinese study , it was
shown that berberine, administered 500 mg twice per day for 3 months, reduced
serum cholesterol by 29%, triglycerides by 35% and LDL-cholesterol by 25%. The
apparent mechanism is increasing the production of a receptor protein in the liver
that binds the LDL-cholesterol, preparing it for elimination.
Research
on use of berberine for diabetes began with Ni Yanxi and his colleagues in Changchun
(a large city in Jilin Province) with diabetes treatments. As an introduction
to a 1995 English language publication on this subject (presenting their earlier
clinical data from 1983-1987), they wrote : "It was found by accident that
berberine had the therapeutic effect on the decrease of blood glucose when the
authors used berberine to treat diarrhoea in patients who suffered from diabetes."
Dietary therapy
was first introduced to the patients for one month. For those who still had high
fasting blood sugar, berberine was administered orally at a dose of 300, 400,
or 500 mg each time, three times daily, adjusting the dosage according to the
blood glucose levels; this treatment was followed for 1-3 months. A control group
without diabetes was similarly treated, with no effect on blood sugar. For the
diabetic patients, it was reported that patients had less thirst, consumed less
water and urinated less, had improved strength, and had lower blood pressure;
the symptoms declined in correspondence with declining blood glucose levels. Laboratory
studies suggest that berberine may have at least two functions in relation to
reducing blood sugar: inhibiting absorption of sugars from the intestine and enhancing
production of insulin. As relayed by Ni in his review of the literature, clinical
experience with berberine has shown that doses of 2 grams per day produced no
side effects.
An
evergreen shrub growing to 3.5m at a medium rate. It is hardy to zone 6 and is
not frost tender. It is in leaf all year, in flower in May. The flowers are hermaphrodite
(have both male and female organs) and are pollinated by Insects. The plant is
self-fertile. We rate it 4 out of 5 for usefulness
The
plant prefers light (sandy), medium (loamy) and heavy (clay) soils and can grow
in heavy clay and nutritionally poor soils. The plant prefers acid, neutral and
basic (alkaline) soils. It can grow in semi-shade (light woodland) or no shade.
It requires dry or moist soil.
Fruit
- raw or cooked. A well - flavoured fruit, it has a sweet taste with a blend of
acid, though there is a slight bitterness caused by the seeds. The fruit is much
liked by children,. It is dried and used like raisins in India. The fruit contains
about 2.3% protein, 12% sugars, 2% ash, 0.6% tannin, 0.4% pectin. There is 4.6mg
vitamin C per 100ml of juice.The fruit is about 7mm x 4mm - it can be up to 10mm
long. Plants in the wild yield about 650g of fruit in 4 pickings.
The
dried stem, root bark and wood are alterative, antiperiodic, deobstruent, diaphoretic,
laxative, ophthalmic and tonic (bitter). An infusion is used in the treatment
of malaria, eye complaints, skin diseases, menorrhagia, diarrhoea and jaundice.
Berberine,
universally present in rhizomes of Berberis species, has marked antibacterial
effects. Since it is not appreciably absorbed by the body, it is used orally in
the treatment of various enteric infections, especially bacterial dysentery. It
should not be used with Glycyrrhiza species (Liquorice) because this nullifies
the effects of the berberine. Berberine has also shown antitumour activity.
Prefers
a warm moist loamy soil and light shade but it is by no means fastidious, succeeding
in thin, dry and shallow soils. Grows well in heavy clay soils.
Plants are
very hardy, they survived the severe winters of 1986-1987 without problems in
most areas of Britain[K].
Plants
can be pruned back quite severely and resprout well from the base
The fruits
are sometimes sold in local markets in India.
Hybridizes
freely with other members of this genus. Most plants cultivated under this name
are B. chitria., B. coriaria., B. glaucocarpa. and, more commonly, B. floribunda.
Seed - best
sown as soon as it is ripe in a cold frame, it should germinate in late winter
or early spring. Seed from over-ripe fruit will take longer to germinate. Stored
seed may require cold stratification and should be sown in a cold frame as early
in the year as possible. When they are large enough to handle, prick the seedlings
out into individual pots and grow them on in the greenhouse or cold frame for
at least their first winter. Once they are at least 20cm tall, plant them out
into their permanent positions in late spring or early summer, after the last
expected frosts. The seedlings are subject to damping off, so be careful not to
overwater them and keep them well ventilated.
Cuttings
of half-ripe wood, July/August in a frame. Very difficult, if not impossible.
Cuttings
of mature wood of the current season's growth, preferably with a heel, October/November
in a frame. Very difficult, if not impossible.